Bizzell Releases Essential Opioid Overdose Response Video in Wake of National Crisis
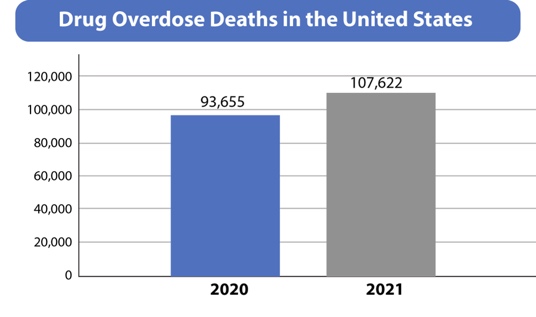
January 22, 2024, New Carrollton, Maryland – As the opioid crisis continues to devastate communities with over 136 American deaths daily, primarily from fentanyl-laced drugs, Bizzell US (Bizzell) has developed and unveiled a vital educational tool. The company has released “Opioid 5 Steps to Respond to Opioid Overdose,” a video outlining critical steps to respond to an opioid overdose, developed under the guidance of leading experts in the field.
The video’s creation was informed by the extensive knowledge and experience of Bizzell’s team of specialists, including experts in health and human services, behavioral health, public health, substance use disorders, treatment and prevention, maternal and child health, medication-assisted treatment, mental health, and pharmacy operations. This collective expertise ensures that the video is not only informative but also grounded in the latest research and best practices.
Anton C. Bizzell, MD, Chairman and CEO, William H. Scarbrough, III, PhD, and Todd W. Mandell, MD are among some of notable experts at Bizzell who contributed their insights, reflecting decades of experience in fields relevant to opioid crisis management, behavioral health, and substance use disorders. Their involvement underscores Bizzell’s commitment to leveraging deep expertise in tackling this pressing public health issue.
This initiative is part of Bizzell’s broader effort to educate and empower individuals and communities in the fight against the opioid epidemic. The video is mandatory viewing for all Bizzell employees and is accompanied by a call to action to carry naloxone (Narcan), an effective emergency response medication now available over the counter.
The educational video will also be accessible on the Bizzell and the Behavioral Health Advancement Resource Center (BHARC) website, forming part of an informative mini-series on the opioid crisis.
About Bizzell US
Bizzell is a strategy, consulting, investment, & technology firm headquartered in New Carrollton, Maryland. Bizzell is a partner of choice for federal, state, and local government agencies, and private organizations. With a strong emphasis on innovation and impact, Bizzell transforms small ideas into powerful catalysts that drive change across markets worldwide. Learn more at www.BizzellUS.com.
About Behavioral Health Advancement Resource Center (BHARC)
Bizzell established the Behavioral Health Advancement Resource Center (BHARC) to provide expert information and resources to support the behavioral health community. With BHARC, Bizzell disseminates new ideas, tools, and solutions to critical behavioral health issues including the opioid epidemic, substance use disorders, suicide prevention, and more. As a leader in behavioral health initiatives, we bring together subject matter experts with exceptional experience, as well as commitment to behavioral health solutions.
For more information, visit www.bharc.org.